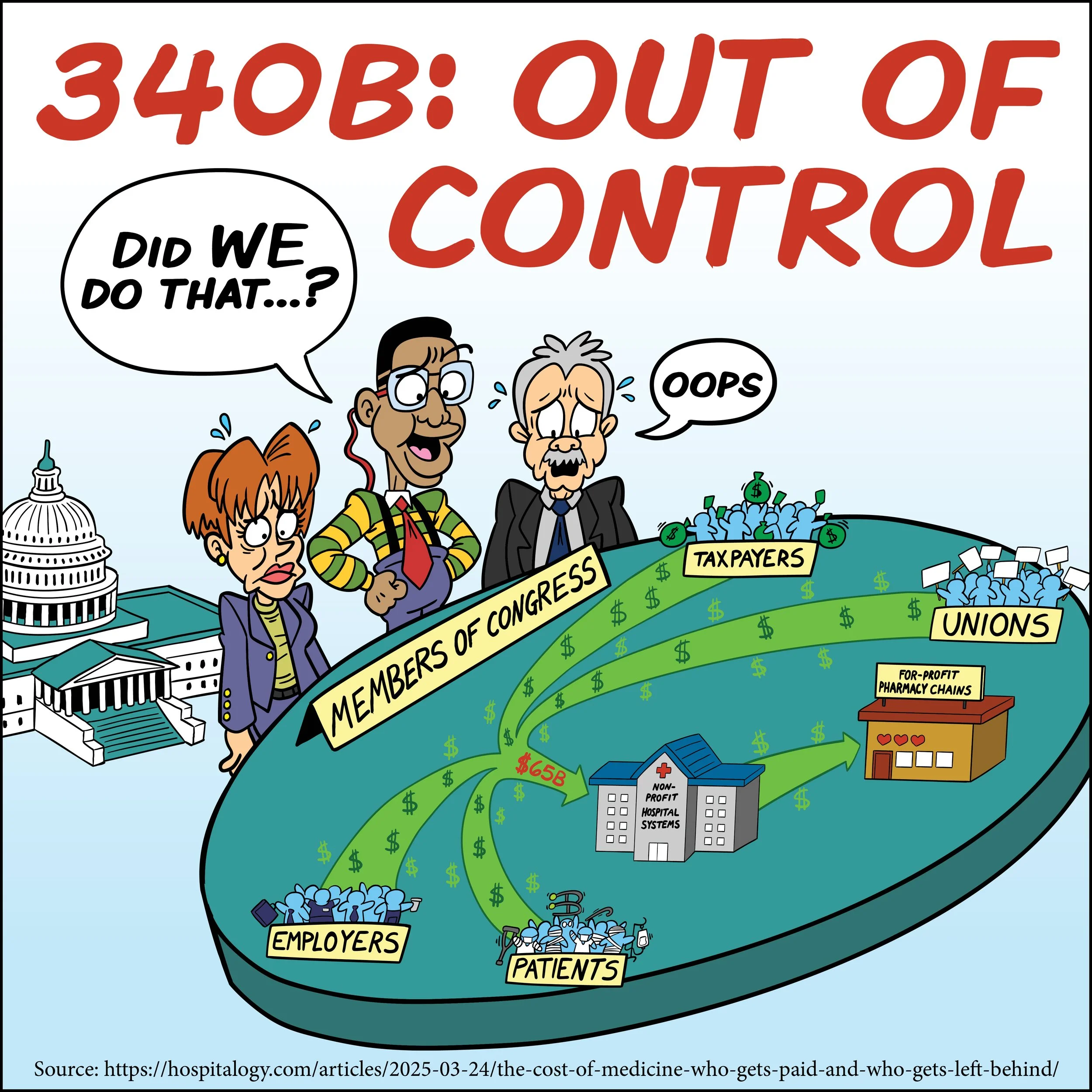
New TAPP Cartoon: 340B Is a Big “Oops” That Needs Fixing
The Trade Alliance to Promote Prosperity has created a new editorial cartoon to illustrate a big “oops” by Congress: The 340B drug pricing program. Congress created the 340B program in 1992 with a genuinely noble purpose: help hospitals and clinics serving low-income Americans stretch limited resources and provide more care to vulnerable patients.
At the time, lawmakers worried that changes to Medicaid drug rebate rules would unintentionally raise pharmaceutical costs for safety-net providers. So, Congress stepped in and required drug manufacturers to provide steep discounts on outpatient medications to certain hospitals and clinics. The idea was simple enough: hospitals serving the poor could buy drugs at discounted rates and use the savings to improve care.
But somewhere along the way, the program drifted far from its original mission.
What was intended as a targeted safety-net policy has evolved into one of the most opaque and controversial corners of the American health care system. Today, the 340B program has ballooned into an enormous enterprise with prescription purchases exceeding $80 billion annually and tens of thousands of participating sites nationwide.
To be fair, Congress probably never envisioned this outcome.
Lawmakers did not foresee massive hospital consolidation driven in part by 340B incentives. They likely did not anticipate sprawling health systems buying up physician practices simply to convert them into 340B-eligible locations. Nor did they expect hospitals to partner with vast networks of contract pharmacies located far from the low-income communities the program was designed to help.
Yet that is exactly what happened.
Under the current structure, hospitals can purchase drugs at sharply discounted 340B prices while billing insurers and patients at full price — keeping the spread as revenue. In theory, those savings are supposed to support charity care and community health services. In practice, however, there is remarkably little transparency about where the money actually goes.
That lack of oversight has created enormous skepticism.
Critics argue that many hospitals now treat 340B less like a safety-net tool and more like a revenue stream. Research organizations and policy analysts have warned that the program’s incentives encourage hospital consolidation, increase outpatient drug costs, and allow large health systems to profit without demonstrating meaningful benefits to poor or uninsured patients.
Even the program’s administration has become a legal and regulatory mess.
The financial burden ultimately falls on patients, employers, unions, and taxpayers.
None of this means the original idea behind 340B was wrong.
Many rural hospitals and genuine safety-net providers still rely on the program to keep services available in underserved communities. Supporters rightly note that the discounts can help hospitals maintain access to care for vulnerable populations.
But good intentions are not enough.
Congress created 340B to help struggling patients — not to create opaque financial incentives that reward consolidation, fuel litigation, and enrich large hospital systems with minimal accountability. What began as a well-intentioned fix has become a sprawling, confusing, and poorly supervised program that no longer consistently serves its original purpose.
That does not mean 340B should be abolished. It means it should be reformed.
Washington needs to restore transparency, tighten eligibility standards, ensure savings actually benefit patients, and return the program to the safety-net mission that Congress originally intended. Until that happens, 340B will remain a cautionary tale of how well-meaning government programs can spiral into dysfunction when oversight fails to keep pace with the program’s mission. Oops!